Category: Injury Prevention
Start them young – Outline for youth resistance training: the 2014 International Consensus Position Statement
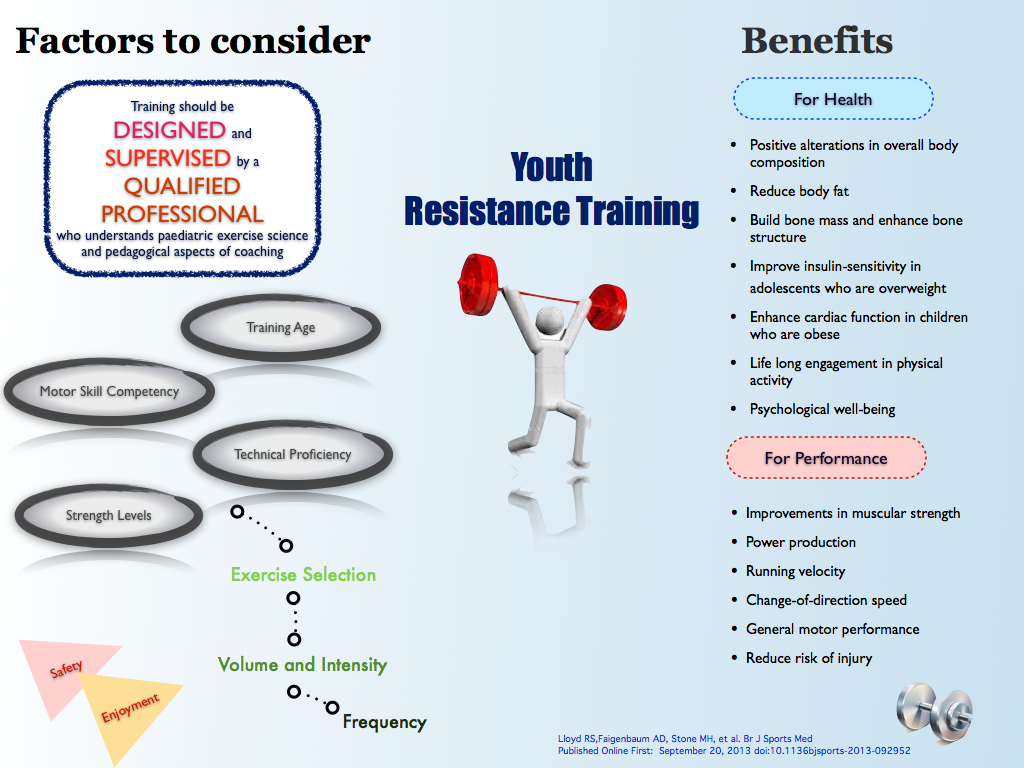
For guidelines on developing athletes over the long term the Youth Physical Development Model by Lloyd and Oliver is a good starting point.
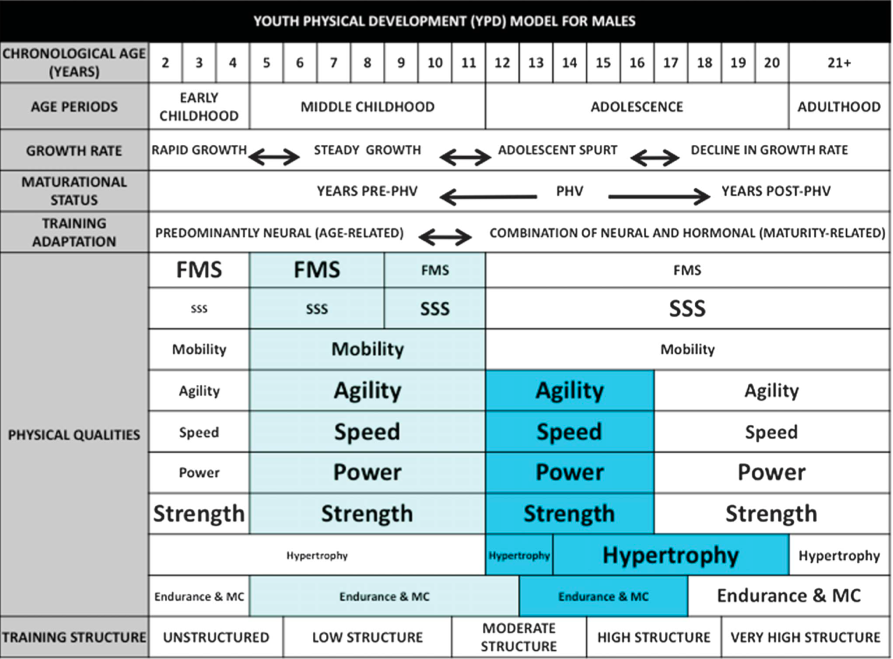
Below are guidelines outlined for males and females.
Males
Females
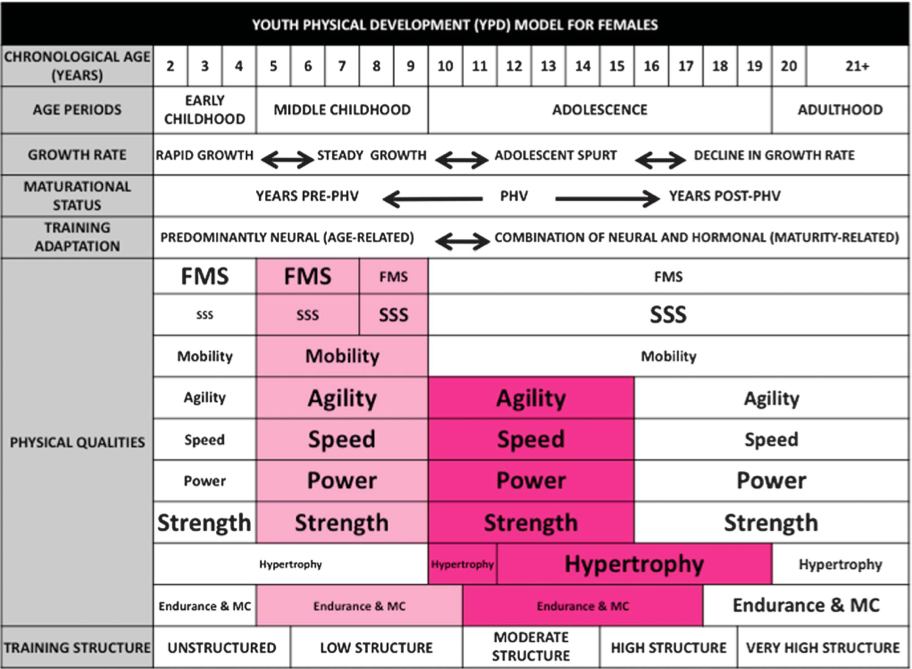
Font size refers to importance
Light blue boxes for males and light pink boxes for females refer to preadolescent periods of adaptation
Dark blue boxes for males and dark pink boxes for females refer to adolescent periods of adaptation.
FMS = fundamental movement skills
MC = metabolic conditioning
PHV = peak height velocity
SSS = sport-specific skills
YPD = youth physical development.
Note, these are guidelines, and ideally programs should individualised according to the factors outlined above.
References:
Lloyd R, Oliver JL. The youth physical development model: A new approach to longterm athletic development. Strength & Condit J 2012;34(3):61-72.
Lloyd RS,Faigenbaum AD, Stone MH, et al. Br J Sports Med. Published Online First: September 20, 2013 doi:10.1136bjsports-2013-092952
Enhancing sports injury prevention research
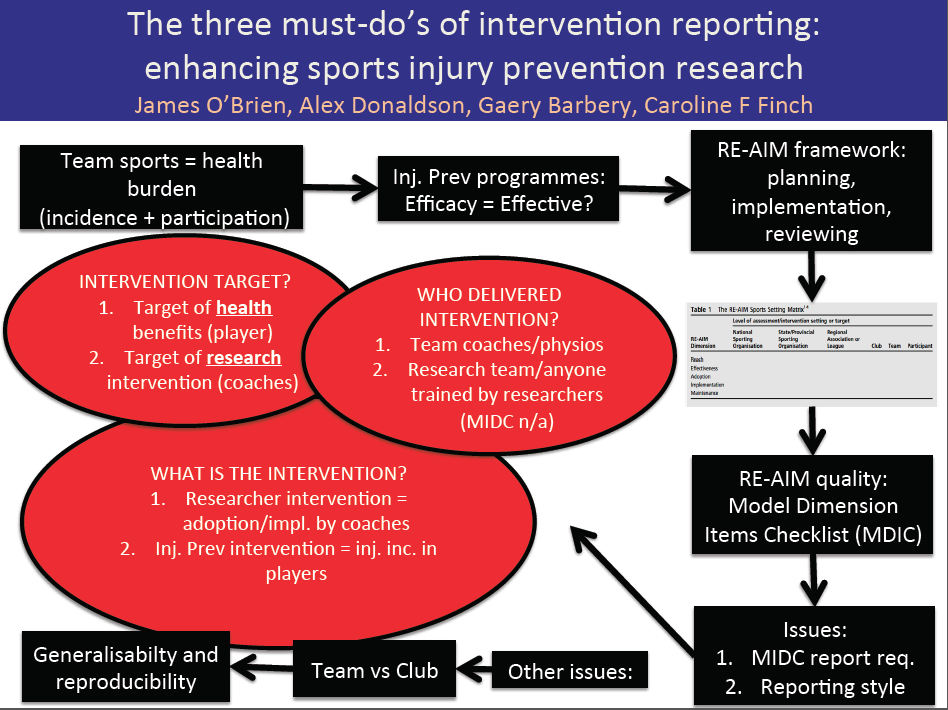
Figure 1. A summary of the editorial “The three must-do’s of intervention reporting: enhancing sports injury prevention research” by O’Brien et al.
Using Figure 1, we attempted to summarise the recent editorial from intervention experts James O’Brien, Alex Donaldson, Gaery Barbery and Caroline Finch from the Centre for Healthy and Safe Sport (CHASS) at the University of Ballarat, Australia in this post. Their article was entitled: “The three must-do’s of intervention reporting: enhancing sports injury prevention research” and was featured in the September addition of the British Journal of Sports Medicine 1. Although it was not in the original article, we have used BokSmart 2 (www.boksmart.com) as an example of an injury prevention programme, simply for the purposes of practical explanation. BokSmart is a nationwide injury prevention programme for Rugby that is being implemented by the South African Rugby Union (SARU). By educating coaches and referees, the programme aims to reduce catastrophic injuries in players.
In our opinion, the take home message of this editorial was that if you would like your intervention to be reproducible and generalisable – and this is an obvious goal of any quality researcher or programme evaluator – your evaluation needs to be very clear in its reporting.
While there are established frameworks such as “Reach, Effectiveness, Adoption, Implementation and Maintenance” (RE-AIM) and checklists such as “Model Dimensions Items Checklist” (MDIC) in place to plan, implement and evaluate injury prevention programmes 1,3, the reporting of these evaluations is often ambiguous, which hinders reproducibility and generalisability. This ambiguity can be reduced by ensuring three questions are answered during your reporting:
1. Who is the intervention target?
- BokSmart is an example of indirect intervention: coaches and referees are the actual target of the intervention (SARU educates them, not the players), and yet the players are targeted, albeit indirectly, for the health benefits (reduction in catastrophic injuries) of the intervention.
- When reporting on the “participants” of the intervention, as the MDIC (checklist) requires, one needs to be clear and distinguish between the targeted health beneficiaries (players, in this case), and the target of the actual intervention (coaches and referees, in this case) if those are two distinct groups – as they are in BokSmart.
2. What is the intervention?
- In the example of BokSmart, there are two levels of interaction occurring simultaneously: one between SARU and the coaches/referees (termed “researcher intervention”) and one between the coaches/referees and the players (termed “injury prevention intervention”).
- The outcome measures or evaluations are very different for these two groups: in the researcher intervention (coaches and referees, in this case) the most appropriate assessment is the adoption and implementation (“A” and “I” of RE-AIM) of the programme in these groups, while in the injury prevention intervention (players, in this case) the most appropriate outcome measure would be changes in injury rates in the players (“E” of RE-AIM).
3. Who delivered the intervention and were they under researcher control?
- Whoever provides the intervention to the health beneficiary (players in this case) is/are termed the “delivery agents” (coaches and referees, in this case). – there is an entire section dedicated to this group in the MDIC.
- If the “delivery agents” are already affiliated with teams prior to receiving the intervention (as in the case of BokSmart), then they function very differently to “delivery agents” who are specifically trained for the intervention and then assigned to teams. This latter category of delivery agents are more like an extension of the intervention team, and should thus be evaluated and reported on differently.
Besides these three important aspects the other term that can cause confusion is the distinction between “teams” and “clubs”. A coach or coaching staff are associated with, and thus have control over, one team. A club may consist of many teams and coaches.
Therefore, if one is to advertise/“show off” one’s particular injury prevention intervention to the rest of the world, one needs to be very clear to not only stick to the established frameworks and checklists, but also to answer the most important questions about the intervention:
WHO is/are the target(s)? WHAT is the intervention? Who DELIVERED the intervention?
REFERENCES:
1. O’Brien J, Donaldson A, Barbery G, Finch CF. The three must-do’s of intervention reporting: enhancing sports injury prevention research. British Journal of Sports Medicine 2013;
2. Viljoen W, Patricios J. BokSmart – implementing a National Rugby Safety Programme. British Journal of Sports Medicine 2012;46:692–3.
3. Finch CF, Donaldson A. A sports setting matrix for understanding the implementation context for community sport. British Journal of Sports Medicine 2010;44:973–8.
A comprehensive analysis of senior men’s professional injury studies in Rugby Union

Poster was presented by Sean Williams at ECSS 2013 held in Barcelona
The aim of this meta-analysis was to summarise existing literature relating to injuries in professional Rugby Union, and to determine the effect of factors such as playing level, playing position and match quarter.
The results confirm that incidence rates in professional Rugby Union can be considered high in comparison to some team sports (e.g. soccer), but are similar to other collision sports (e.g. rugby league and ice hockey).
The incidence rate in the first quarter of matches was substantially lower than other match periods, suggesting that fatigue may have an important role to play in match injury risk.
Around 12% of injuries were recurrences, and these were typically more severe than new injuries.However, it should be noted that no studies have directly compared the severity of recurrent injuries to their index injuries; it may be that some types of injury are more likely to reoccur, and if these tend to result in substantial time-loss then the recurrent injury severity figure may be skewed. This warrants investigation in future studies.
Injuries most commonly occur during the tackle, and the lower limb is the body region with the highest injury incidence; both of these areas may be targets for future injury prevention strategies.
This summary was written by the first author of the paper, Sean Williams.
You can find the full article http://link.springer.com/article/10.1007/s40279-013-0078-1
Sean Williams is a rugby science postgraduate student at the University of Bath, in the Department of Sport, Health and Exercise Science for Health.
You can contact Sean at S.Williams@bath.ac.uk or follow him on twitter @sw356.
